2021 VOL. 8, No. 2
Abstract: COVID-19 provided an opportunity to experiment with alternative delivery mechanisms for a medical education programme offered through open and distance learning with face-to-face training as an essential component of the programme. Non-availability of hard copies of the course material (92%) and lack of communication from the university (32%) as well as training centres (42%) were some of the challenges faced by students of the Geriatric Medicine programme of the Indira Gandhi National Open University (IGNOU) during the COVID pandemic. Around 90% were willing to attend online classes and 65% to 77% were willing to present cases online for discussion. A programme-specific web portal containing all resource material and information was visited by 85% of students. Most students attended the online classes and 68% attempted the formative assessments based on the online classes. Online classes were recorded and uploaded and were found useful by 90% of students. The experiment successfully demonstrated the feasibility and acceptance of delivering practical skills using online technological tools. Further integrating technology to complement some of the face-to-face component could be used as a permanent and effective delivery strategy, which could also reduce resource requirements.
Keywords: open and distance learning, geriatric medicine, online, COVID.
The sweep of the COVID-19 pandemic brought with it a paradigm change in medical education. Many hospitals in countries across the world were converted into dedicated COVID hospitals resulting in non-availability of regular patients for teaching-learning. The shortages of Personal Protective Equipment (PPE) and the high infectivity of the virus forced medical faculty to avoid including medical students in the clinical teams and rotations (Dedeilia, Sotiropoulos, Hanrahan et al, 2020). There was an apprehension that asymptomatic, infected students might spread the virus. There was also a possibility that they might contact the virus in the course of their training. All these factors, coupled with the guidelines for social distancing by organisations like the Centre for Disease Control (CDC) and World Health Organisation (WHO) experts, concluded that small group discussions and demonstrations to medical faculty would not be possible (Newman & Lattouf, 2020). Medical programmes were thus bound to be severely affected. Since the virus showed no signs of abating, alternative strategies needed to be worked out to ensure that the quality of medical education and training did not suffer.
With the coming of COVID-19, institutions across the world, debated, experimented, shared ideas and put in practice various ICT tools for delivering lectures, student interactions, clinical discussions, presentations and assessment strategies. Didactic lectures were replaced by webinars, electronic conferences also called e-conferences, small and large group meetings (Dedeilia, Sotiropoulos, Hanrahan et al, 2020; Rose 2020; Ish, Sakthivel, Gupta, et al, 2020). Practical skill demonstrations were carried out by simulated patients and technology, videos, augmented and virtual reality. Researchers suggested that counselling and communication skills as well as history-taking skills and systemic examination could be developed with simulated patients, which could then be demonstrated on patients. Problem-specific patient interviewing, disease presentations, and team training are a few other strategies that could be explored and adopted (Centre for Disease Control and Prevention, 2020).
Studies even before the COVID era have also shown that simple online platforms, like websites and blogs, can be used to host videos for demonstrating essential skills, such as procedural clinical skills and communication (Dong & Goh, 2015). Online programmes can also help health professionals from multiple countries to connect and its flexibility ensures better control over learning (Barteit, Guzek, Jahn et al, 2020).
Students were also worried as to how the medical school would be able to make up for the lost practical classes and how they would be prepared to handle emergencies without adequate exposure (Chinelatto, Costa, Medeiros, et al, 2020). Other challenges that the students faced were related to their online assessment and grading, access to computer hardware or software, technical barriers and phobias, little or no experience of online education and pandemic-related anxiety (Rajab, Gazal & Alkattan, 2020; Chinelatto, Costa, Medeiros et al, 2020). Other challenges identified were lack of technical skills, time management, resources available and poor communication at various levels (Nimavat, Singh, Fichadiya et al, 2021). Similar challenges were experienced by students in the transition to online education in non-emergency situations (Rajab et al, 2020; Rosen & Weil, 1995).
Despite these challenges, the COVID-19 pandemic also ushered in new opportunities for teaching and learning. Web-based activities and new teaching technologies were introduced (Rasmussen, Sperling, Poulsen et al, 2020) and for many became the only way of teaching due to isolation protocols (Rose, 2020). Many studies have reported e-learning to be easier and more effective, since it allows access to large quantities of a variety of information and the students can have more control of the educational content since there is a possibility of a personalised approach to learning (Mooney & Bligh, 1997; Ghanizadeh, Mosallaei, Dorche et al, 2018; Chu & Chan, 1998).
This study was undertaken on the geriatric medicine programme of the Indira Gandhi National Open University (IGNOU), India. IGNOU offers continuing medical education programmes through open and distance learning, though an undergraduate first degree is not allowed to be offered at a distance by the respective regulator in the country. These programmes also have a significant portion of the credit load devoted to practical courses, wherein hands-on training in identified medical colleges and hospitals is an essential component of the programme.
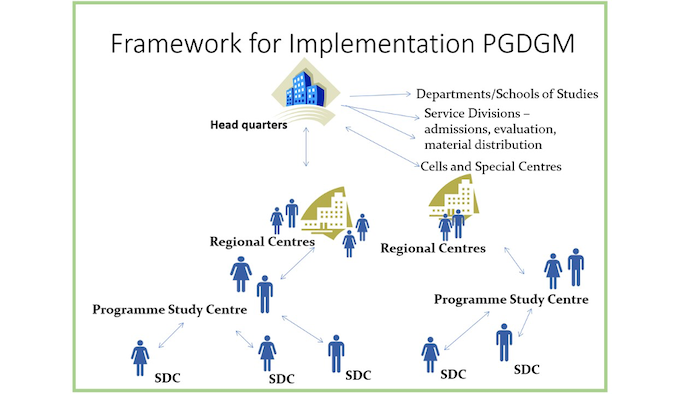
One such programme is the one-year Post Graduate Diploma in Geriatric Medicine programme (PGDGM) for in-service MBBS doctors. Customised printed course material along with course specific videos, teleconferencing and hands-on, face-to-face training are part of the programme package. Part of this training is conducted at identified and notified training centres called Programme Study Centres (PSCs), situated in tertiary level hospitals and medical colleges, which is followed by practice at district level hospitals designated as skill development centres (SDCs). The framework of implementation is depicted in Figure 1.
The students are required to clear both internal assessments and term end assessments to successfully complete the programme.
Figure 1: A framework for implementation of the PGDGM Programme
The coming in of COVID-19 brought about various challenges for the students of the January 2020 session to pursue the programme. These were identified as:
Alternate strategies had to be worked out and put in place to deal with these challenges.
However, before the implementation of the revised strategy could be put in place, it was important to get feedback from the students regarding the feasibility of implementing the strategy.
It was found that although many studies have been carried out to assess the impact of COVID-19 and devise alternative mechanisms for medical education courses offered through the face-to-face mode, there are not many studies conducted on students admitted in open and distance learning courses for medical education. The present study was undertaken against this backdrop and the objectives of the study were set out as follows.
The present research study was undertaken with the following objectives:
This programme presents a strong case for a research study of this kind since IGNOU is one of the few universities in the world offering certified post graduate medical programmes through ODL mode with a significant face-to-face component.
Students enrolling in the medical programmes being offered by IGNOU through ODL mode are a heterogenous group with respect to their age, qualification, experience and employment status, besides differences in other demographic characteristics. It was decided to include the entire batch, since this would enable feedback from all categories of students.
Based on the review of the literature a thematic framework was prepared as in Figure 2. Based on the review of the literature, we constructed a survey comprising a three-part research framework as shown in Figure 2 and used it to find the challenges, enablers and the acceptability of technology enabled delivery of medical programmes.
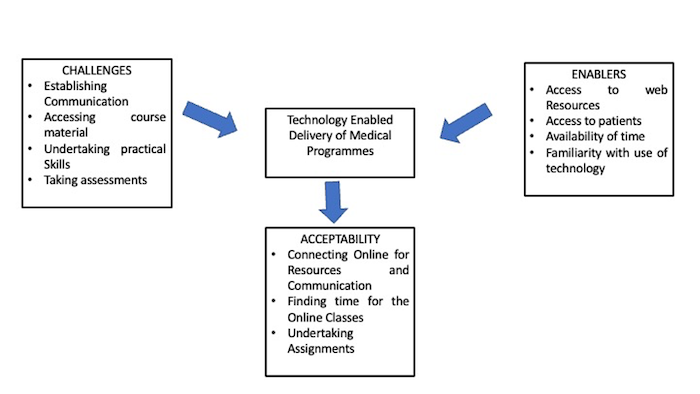
Figure 2: Technology enabled delivery of medical programmes' research framework
Both qualitative as well as quantitative data was required to achieve the objectives set out for the research. It was decided to adopt the survey method for data collection. This ensured a quick and cost-effective way of gathering information.
Emails were sent to all the students admitted in January 2020 to identify the different challenges faced by the students and enablers for a revised implementation strategy. Students whose email addresses were found to be incorrect were contacted by phone and their email information corrected. All students who had filled out the registration form for admission to the programme were contacted and, based on the feedback of the students and discussions with the programme managers in charge of the programme study centres, a revised implementation strategy was worked out and put in place. The managers in charge of the programme study centres where the programme had been activated were involved in the discussions. These included centres like Maulana Azad Medical College Delhi, SN Medical College Jodhpur, MGM Medical College Wardha, B J Medical College Pune, MS Ramaiah Medical college and Hospitals Bangalore, Banaras Hindu University Varanasi, Medical College & Hospital Kolkata, and CMC Ludhiana. After implementing the revised strategy, feedback was again taken from the students to assess the acceptance of the revised strategy. In the second review, 73 students were contacted (those who had responded in the first review). Out of these 57 responded in the second review.
The entire population of students who had registered for admission in the programme in January 2020 Session were taken as the sample. This amounted to 82 students. The questionnaire was sent to all the students. However only 73 responded. For the second review, the questionnaire was sent to the 73 students who had responded in the first review, since the rest of the students (nine) had not responded despite repeated requests. Fifty-seven out of the 73 students who were sent the questionnaire responded.
A questionnaire was developed for taking all the feedback using Google forms because of the ease of filling and collecting responses. The questions included both structured and open-ended question. The questionnaire was reviewed and validated by the subject experts and distance education experts. The reliability of the questionnaire was checked by asking a sample of the students to fill out the questionnaire and repeating with the same set of students after 15 days. After the questionnaires were checked for validity and reliability they were administered to the students. The students were sent two reminders on two consecutive weekends through mail and regular follow up on the WhatsApp group over a 15-day period for getting maximum responses.
The sample characteristics of the entire population was taken from the registration data obtained from the Student Registration Division of IGNOU.
Table 1: Characteristics of the students and respondents of the survey — January 2020 batch |
|||||||
Characteristic |
Sub type of Characteristic |
Admission data 2020* |
% of admission data 2020 |
Response to Questionnaire for enablers** |
Response to Questionnaire for enablers (%) |
Response to Questionnaire for acceptance of revised implementation strategy*** |
Percentage |
1955-1959 |
2 |
2 |
2 |
3 |
2 |
4 |
|
1960-1964 |
4 |
5 |
4 |
5 |
3 |
5 |
|
1965-1969 |
5 |
6 |
4 |
5 |
5 |
9 |
|
1970-1974 |
4 |
5 |
4 |
5 |
4 |
7 |
|
1975-1979 |
7 |
9 |
6 |
8 |
6 |
9 |
|
1980-1984 |
9 |
11 |
7 |
10 |
6 |
11 |
|
1985-1989 |
23 |
28 |
21 |
29 |
17 |
29 |
|
1990-1994 |
24 |
29 |
21 |
29 |
12 |
22 |
|
1995-1999 |
4 |
5 |
4 |
5 |
2 |
4 |
|
Gender |
Male |
52 |
63 |
46 |
63 |
31 |
53 |
Female |
30 |
37 |
27 |
37 |
26 |
47 |
|
Year of completion of Internship |
1975-1979 |
1 |
1 |
1 |
1 |
1 |
2 |
1980-1984 |
1 |
1 |
1 |
1 |
1 |
2 |
|
1985-1989 |
3 |
4 |
3 |
4 |
3 |
5 |
|
1990-1994 |
5 |
6 |
4 |
5 |
5 |
9 |
|
1995-1999 |
3 |
4 |
3 |
4 |
3 |
5 |
|
2000-2004 |
10 |
12 |
9 |
12 |
8 |
13 |
|
2005-2009 |
5 |
6 |
4 |
5 |
3 |
5 |
|
2010-2014 |
20 |
24 |
17 |
23 |
15 |
25 |
|
2015-2019 |
34 |
41 |
31 |
42 |
18 |
33 |
|
Marital Status |
Married |
57 |
69 |
50 |
68 |
41 |
74 |
Unmarried |
25 |
31 |
23 |
32 |
15 |
26 |
|
Employment Status |
Employed |
56 |
68 |
52 |
71 |
36 |
64 |
Unemployed |
26 |
32 |
21 |
29 |
21 |
36 |
|
Total |
|
82 |
100 |
73 |
100 |
57 |
100 |
*Information obtained from the registration data of the university for the January 2020 admission of PGDGM programme
**Information obtained from the first questionnaire was sent to all the 82 admitted students
*** Information obtained from the second questionnaire was sent to the 73 students who responded to the first questionnaire
Eighty-two students enrolled for the January 2020 batch and 73 (69.5%) students filled in the first feedback form sent in June 2020. Fifty-seven (69% of the admitted students and 78% of the students who responded to the first questionnaire) responded to the second feedback form sent in August 2020. The characteristics of the admitted students, students who filled in the questionnaire in June and those who filled in the form in August is presented in Table 1.
About 66% of the enrolled students were more than 20 years of age, the maximum being in the range of 20 to 25 years. Sixty-three percent of the admitted students were males. About 40 percent of the students had completed their internship within the last five years. Around 60% of the students were married and 60% were employed.
A Chi-square test of the category-wise responses revealed that there was no notable difference between normal frequencies and observed frequencies in both cases of responses. (Enabler response χ = 0.07, df = 4, p = 9.49 at 0.05 significance level and acceptance response χ = 0.67s, df = 4, p = 9.49 at 0.05 significance level). Thus, this data can be used for further analysis as random data.
About 92% of students had not received hard copies of the course material.
The feasibility of an alternate strategy was assessed by enquiring about a few enablers through the questionnaire. The enablers and responses of the students to these enablers is presented in Table 2.
A programme-specific web portal had been created for the students in July 2020 and soft copies of the material, resource material and programme guide were made available to the students. The access for the web portal by the students for accessing various resource was considered as an enabler.
A majority of the students (83.8%) were able to access the web portal. A good number (77%) could download the soft copy of the course material and about 30% attempted the assignments. The reference videos posted were viewed by 29.7% of the students.
Table 2: The enablers and responses of the students for revised implementation strategy
| Enablers | Response to Enablers |
Number of Students |
Percentage |
Access to Web portal |
Yes |
62 |
85 |
Did not try |
7 |
10 |
|
No |
4 |
5 |
|
Downloaded the course material from the web portal |
Yes |
57 |
78 |
Did not try |
11 |
15 |
|
No |
5 |
7 |
|
Read the course material |
Both theory courses |
13 |
18 |
Only one theory course (basic geriatrics) |
27 |
37 |
|
Only one theory course (clinical geriatrics geriatrics) |
1 |
1 |
|
Did not get time |
19 |
26 |
|
Neither received the hard copies, nor could access soft copies |
13 |
18 |
|
Viewing of reference Videos in web portal |
Yes |
38 |
52 |
No |
35 |
48 |
|
Attempted theory assignments |
Yes |
22 |
30 |
No |
51 |
70 |
|
Workload in service |
Attending to their duty in the hospital every day |
48 |
66 |
Employed in COVID hospitals |
11 |
15 |
|
Were attending work few days a week |
6 |
8 |
|
Were not going for work at all |
5 |
7 |
|
Qualifications |
No post-graduation |
23 |
32 |
Community medicine |
7 |
10 |
|
Medicine |
6 |
8 |
|
Family medicine |
4 |
5 |
|
Other clinical specialisations |
4 |
5 |
|
Pre/paraclinical |
5 |
7 |
|
Readiness to attend the online classes |
Would be able to attend all the web conferencing classes |
44 |
60 |
Would try to attend most of them |
29 |
40 |
|
Was busy and would not be able to attend the classes |
1 |
1 |
|
Availability of elderly to take cases for case presentation |
Could examine elderly in the hospitals visited |
55 |
75 |
Have elderly at home |
48 |
66 |
|
Preferred timing for the classes |
3 pm to 7 pm |
62 |
85 |
Weekdays were not suitable for them |
6 |
8 |
|
after 5 pm |
18 |
25 |
|
Ready to take online exam for theory |
Yes |
60 |
82 |
No |
13 |
18 |
|
Ready to take online exam for practical |
Yes |
49 |
67 |
No |
24 |
33 |
|
Total students |
|
73 |
100% |
Analysis of the enablers revealed that most of the students (60%) were eager to attend all the classes and another 40% mentioned that they would try to attend most of them. The timing of the classes preferred by majority of them was between 3 and 7 pm, especially after 5 pm. A large number of the students (66%) were attending the hospital every day and 15% were posted in COVID hospitals. About 75% mentioned that they would have access to elderly patients for examining and case presentation and 66% had elderly at home who could also be taken for case presentation.
Implementation of the Modified Implementation Strategy
After receiving a positive feedback from the students, it was decided to implement the modified strategy. The demonstrations in the bed side teachings were replaced by online classes through web conferencing using google meet platform. All the live web conferencing classes were recorded and videos of the recorded classes shared with the students. Few of the skills like patient examination and demonstration of signs by the students for which face to face counselling sessions could not be replaced by online methods were reserved for the hand on training to be scheduled in the end of the year, when situation was expected to improve. A vigorous formative assessment component was put in place.
The acceptance of the modified strategy by students was assessed through a feedback form in the month of August 2020 and the results are placed in Table 3.
Table 3: Acceptance of the implementation strategy
| Components of the Programme | Responses by Students Regarding Acceptance |
Number of Responses |
Percentage |
Downloading study material soft copy |
All could download |
57 |
100 |
Requirement of hard copy |
Expressed that hard copy of the material is essential for studying |
54 |
95 |
They could manage only with the soft copy |
2 |
4 |
|
Preferred mode of communication |
31 |
54 |
|
9 |
16 |
||
Web support portal |
7 |
12 |
|
Accessing web support portal |
Regularly visited |
50 |
88 |
Accessed only when they got time |
3 |
5 |
|
Could not, due to lack of time |
3 |
5 |
|
Did not feel the need. |
1 |
2 |
|
Access the course material |
From the web portal |
46 |
81 |
By email |
6 |
11 |
|
From WhatsApp |
1 |
2 |
|
Did not try |
3 |
5 |
|
Not able to |
1 |
2 |
|
Access the log books |
From the web portal |
38 |
67 |
By email |
6 |
11 |
|
From WhatsApp |
5 |
9 |
|
Did not try |
8 |
14 |
|
Web conferencing classes videos |
From the web portal |
47 |
82 |
By email |
6 |
11 |
|
From WhatsApp (two also accessed from email) |
4 |
7 |
|
Did not try |
1 |
2 |
|
Not able to |
3 |
5 |
|
Internal Assessment for videos |
From the web portal |
45 |
79 |
By email |
5 |
9 |
|
From WhatsApp (two also accessed from email) |
3 |
5 |
|
Did not try |
3 |
5 |
|
Not able to |
3 |
5 |
|
Assignments |
From the web portal |
45 |
79 |
By email |
4 |
7 |
|
From WhatsApp (one also accessed from email) |
3 |
5 |
|
Did not try |
2 |
4 |
|
Not able to |
4 |
7 |
|
Reference material |
From the web portal |
31 |
54 |
By email |
2 |
4 |
|
From WhatsApp (two also accessed from email) |
1 |
2 |
|
Did not try |
16 |
28 |
|
Not able to |
6 |
11 |
|
Did not know of its existence |
1 |
2 |
|
Reference audio video |
From the web portal |
37 |
65 |
By email |
4 |
7 |
|
From WhatsApp (one also accessed from email) |
3 |
5 |
|
Did not try |
10 |
18 |
|
Not able to |
3 |
5 |
|
Did not know of its existence |
1 |
2 |
|
Attempting theory assignments |
Attempted |
28 |
49 |
Attending classes |
Attended all the classes |
21 |
37 |
Attended some and viewed recorded videos of the missed classes. |
33 |
58 |
|
Attended few classes but had no time to see the videos. |
2 |
4 |
|
Was not attending any class. |
1 |
2 |
|
Submitted formative assessments |
Yes |
40 |
70 |
Few |
12 |
21 |
|
None |
5 |
9 |
|
Reasons for not submitting formative assessment |
Did not get time to do assessments |
9 |
16 |
Could not study for them |
7 |
12 |
|
Not able to access |
1 |
2 |
|
Feedback on formative assessments |
They were from the subject taught in the class |
35 |
61 |
They helped understand and remember the subject |
33 |
58 |
|
Some were ambiguous |
13 |
23 |
|
Easy |
3 |
5 |
|
Difficult |
5 |
9 |
|
Recorded videos of web conferencing classes |
Very useful resource |
55 |
96 |
Did not get time to go through |
4 |
7 |
|
Total |
|
57 |
100 |
A good number of students (88%) could access the web portal and used it for downloading the course material, logbooks, web conferencing classes videos and assessments. Most of them preferred WhatsApp for communication. The videos were found to be very useful by 96% of students. More than 90% tried to attend most of the classes and 70% submitted the assignments for practical classes.
A proposed model for delivery of the medical education programmes through the blended approach is shown in Figure 3.
The skills to be imparted for any medical programme include all the three domains — cognitive, affective and psychomotor.
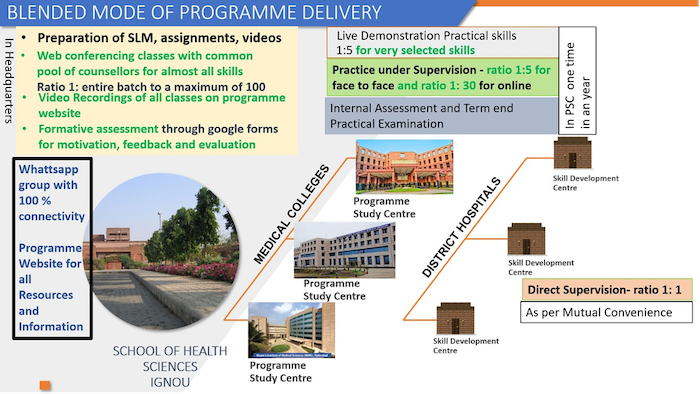
Figure 3: A proposed model for delivery of medical education programmes
through the blended approach
The skills related to the cognitive domain can be imparted through course material which is developed in a self-instructional or self-learning style. The content is presented in a simple and conversational style for enhancing the understanding of the learner and contains access devices in the form of in-text questions with readily available answers, glossaries or key words and a summary at the end to help reinforce the concepts. A few of the skills related to the affective domain can also be covered through these self-instructional materials. Web conferencing classes and discussion forums at dedicated websites can be resorted to in order to supplement the course materials and bridge the gap between the students and their teacher. This not only allows for synchronous and asynchronous interactions between the teacher and students but also an interaction between peers.
Few psychomotor skills, that need to be demonstrated by the counsellors, can be taken up through the web conferencing mode. Those requiring the manipulation and replication of skills related to physical contact or handling of the patient and requiring face-to-face interactions by the students, can be undertaken under the supervision of teachers or counsellors in the designated programme study centres housed in medical colleges and big teaching hospitals. To ensure adequate practice and proficiency in the development of skills without displacing the learners too much from their place or work, the learners are required to practise their skills acquired at the PSC in the district hospitals (SDCs).
Thus, making use of technology and integrating it with the essential face-to-face hands-on training of skills would provide an effective, low-cost model for training a large number of medical graduates, without displacing them from their workplace for long periods of time.
This study brings to light many important findings that can be used to plan a blended approach for medical education. It highlights the advantages of delivery of part of the practical training through online-mode demonstrations of skills by counsellors, case discussion by students, and reading of investigations like ECG, X-ray, etc. Inputs in the form of videos which can be viewed by the students at their own pace and within their own time frame, any number of times as required, make the learning more permanent and effective. This is also a very useful resource for slower learners and also those who tend to fall back into a conventional system. This study has demonstrated that videos are a much-visited resource by the students in an e-learning environment. The repeated reinforcements subjected to volunteering by the students can help boost the confidence of students and build a very strong base which will help them when they come for hands-on training in a face-to-face environment for practice of the skills demonstrated in the online classes. The regular formative assessments also play an important role in reinforcing learning. They not only provide motivation but also are a means of self-assessment and monitoring of students’ understanding of and the progress in the course. A blended approach can thus integrate the advantages of face-to-face hands-on training of the skills, which is an essential component of all medical education training programmes, with an online component that can serve to reinforce learning and provide a strong supplement to the practical component. Medical educators would need to reorient their strategies of teaching learning and design their programmes accordingly.
Based on the findings of this study, we would proffer the following practical recommendations that should be of use to any institution considering medical education through the blended approach as a teaching–learning strategy.
The study also leads us to think (and rethink) about the role strategic planning of medical training plays in the acceptance of modes of training. IGNOU is a technology leader in education and also the largest open university in the world. It is thus natural for the university to progress in the direction of virtualisation and provide access to its huge academic resources to clients across the globe. This is an area for all distance teaching institutions to consider further reflection and collaborative R&D for creating common resources and platforms for learning.
Centers for Disease Control and Prevention. (2020). Standard Operating Procedure (SOP) for triage of suspected COVID-19 patients in non-US healthcare settings: Early identification and prevention of transmission during triage. https://www.cdc.gov/coronavirus/2019-ncov/hcp/non-us-settings/sop-triage-prevent-transmission.html
Chinelatto, L. A., Costa, T. R. D., Medeiros, V. M. B., Boog, G. H. P., Hojaij, F. C., Tempski, P. Z., & Martins, M. D. A. (2020). What you gain and what you lose in COVID-19: Perception of medical students on their Education. Clinics, 75.
Chu, L. F., & Chan, B. K. (1998). Evolution of web site design: Implications for medical education on the Internet. Computers in Biology and Medicine, 28(5), 459-472.
Dedeilia, A., Sotiropoulos, M. G., Hanrahan, J. G., Janga, D., Dedeilias, P., & Sideris, M. (2020). Medical and surgical education challenges and innovations in the COVID-19 era: A systematic review. in vivo, 34(3 suppl), 1603-1611.
Dong, C., & Goh, P. S. (2015). Twelve tips for the effective use of videos in medical education. Medical Teacher, 37(2), 140-145.
Ghanizadeh, A., Mosallaei, S., Dorche, M. S., Sahraian, A., & Yazdanshenas, P. (2018). Attitude and use of e-learning, education by medical students in Shiraz, Iran. Internal Medicine and Medical Investigation Journal, 3(3), 108-111.
Mooney, G. A., & Bligh, J. G. (1997). Information technology in medical education: Current and future applications. Postgraduate Medical Journal, 73(865), 701-704.
Newman, N. A., & Lattouf, O. M. (2020). Coalition for medical education—A call to action: A proposition to adapt clinical medical education to meet the needs of students and other healthcare learners during COVID‐19. https://onlinelibrary.wiley.com/doi/full/10.1111/jocs.14590
Nimavat, N., Singh, S., Fichadiya, N., Sharma, P., Patel, N., Kumar, M., ... & Pandit, N. (2021). Online medical education in India—Different challenges and probable solutions in the age of COVID-19. Advances in Medical Education and Practice, 12, 237.
Rajab, M. H., Gazal, A. M., & Alkattan, K. (2020). Challenges to online medical education during the COVID-19 pandemic. Cureus, 12(7).
Rajab, M. H., Gazal, A. M., Alkawi, M., Kuhail, K., Jabri, F., & Alshehri, F. A. (2020). Eligibility of medical students to serve as principal investigator: An evidence-based approach. Cureus, 12(2).
Rasmussen, S., Sperling, P., Poulsen, M. S., Emmersen, J., & Andersen, S. (2020). Medical students for health-care staff shortages during the COVID-19 pandemic. The Lancet, 395(10234), e79-e80.
Rose, S. (2020). Medical student education in the time of COVID-19. JAMA, 323(21), 2131-2132.
Rosen, L. D., & Weil, M. M. (1995). Computer availability, computer experience and technophobia among public school teachers. Computers in Human Behavior, 11(1), 9-31.
Author:
Ruchika Kuba, MBBS, MD in Preventive and Social Medicine, is a Professor in the School of Health Sciences, IGNOU. Ruchika coordinated the planning development and implementation of many programmes for doctors, dentists and other health functionaries in the areas of health offered through open and distance learning mode. The programmes cover subjects of public health importance like geriatrics, maternal and child health, medical education, waste management, dentistry, patient safety, etc. She initiated and coordinated many national and international projects, training programmes conferences and workshops. Member of Expert Panel for syllabus of MD Geriatric Medicine by MCI. She is also a member of the Standing Committee of Social Justice and Empowerment, Govt. of India for examining “The Maintenance and Welfare of Parents and Senior Citizens Bill, 2007”, a PhD examiner for the University of Delhi and an expert faculty examiner and member of the Expert Review Group for various courses offered by other institutions, such as the Certificate and Post Graduate Certificate of Gerontology courses developed by National Institute of Social Defence, Ministry of Social Justice and Empowerment, GOI, and the Post Graduate Diploma in Health and Social Gerontology course at the Institute of Home Economics, University of Delhi. Ruchika has published articles in books and journals, presented papers and chaired sessions in geriatric conferences. Email: kubaruchika@gmail.com
Cite this paper as: Kuba, R. (2021). Technology enabled delivery of medical programmes through ODL: A study of training medical doctors in geriatric medicine. Journal of Learning for Development, 8(2), 298-311.